

What is a 'First-grader Problem'?
Recently, the term 'first-grader problems' is often used by educationists as well as the wider public. A first-grader problem refers, as the words indicate, to the problematic behavior of children in the first grade of elementary school.
Unlike in kindergarten and daycare centers, children at elementary school are required to sit at desks according to the school time-table and do the same things with others in line with the teacher's instructions. The majority of first-graders feel bewildered at the beginning, but by the end of the first semester, they get used to the school's rules and eventually behave more like an elementary student. However, recently there is an increasing number of first-graders who cannot adapt to such changes and rules; even after a time during which they should have gotten used to the new environment, they are unable to follow the teacher's instructions, wait their turn to speak out, or sit at a desk for a certain number of hours.
The National Institute for Educational Policy Research has coined such phenomena 'first-grader problems' and defined these as follows:
The situation where a child does not follow the teacher's instruction and acts on his/her own in the classroom at the elementary school; as a result, the teacher cannot conduct teaching, and in the end, the function of the school as group education does not work properly for a certain period of time; and such a problem cannot be solved in the usual way by the classroom teacher alone.
("The current situation of and measures for issues concerning school management", the National Institute for Educational Policy Research, 2000)
Why are first-grader problems increasing?
Why do we often hear of first-grader problems nowadays? The National Institute for Educational Policy Research has conducted a survey on the issue, which has revealed several causal factors as shown in Table 1.
The results indicate that the causes of first-grader problems cannot necessarily be attributed solely to children; yet it is still certain that there are some children who have difficulty participating in group activities (see the underlined part in Table 1).
Table 1: Ten situations in which a class does not function properly in school
(The National Institute for Educational Policy Research, 2000)
- Insufficient collaboration between preschool and elementary school teachers;
- Children who need special care and educational assistance;
- Children who do not receive necessary childcare at home;
- Children who dislike the teaching method and content they receive;
- Delay in taking proper action against problematic behaviors such as bullying;
- Lack of the head teacher's leadership or collaboration among teachers;
- Lack of the teacher's flexibility in organizing classes;
- Delay in taking action due to insufficient communication and a failure to establish a relationship between school and parents;
- Failure to utilize the results of research and fieldwork in school; or
- Poor parenting or an improper response from the school.
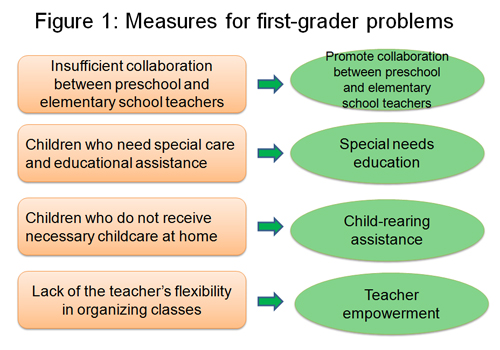
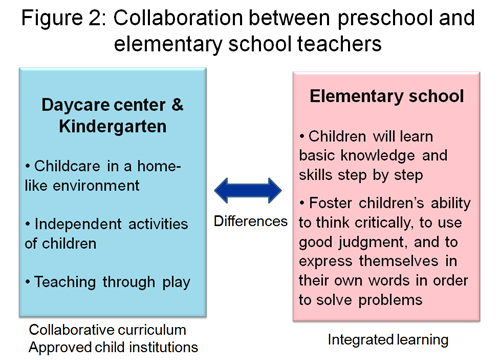
Various measures have been proposed to solve these first-grader problems (Figure 1); in particular, promoting collaboration between preschool and elementary school teachers is widely considered to be useful in helping children make a smooth transition to full-time elementary education (Figure 2).
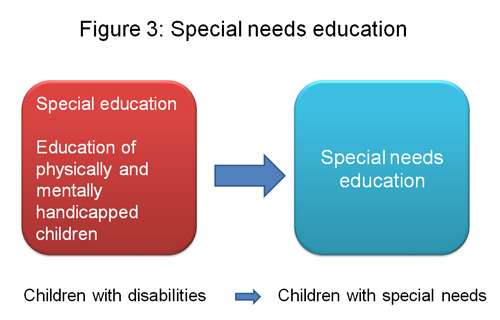
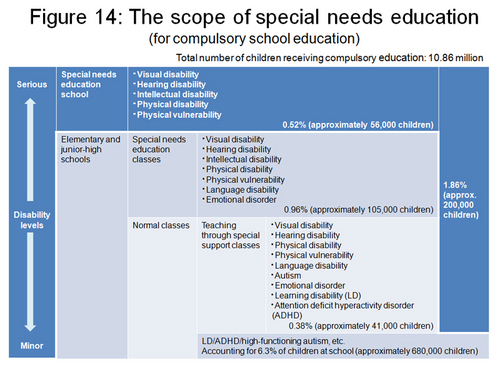
However, there is also another factor that is often identified in children with problems in social development, known as a Developmental Disorder, an innate inability to produce normal behavioral output. Such children have special educational needs and the aforementioned collaborative approach is not sufficient to provide adequate care for them. Traditionally, children with intellectual or physical disabilities receive special care within the framework of 'special education'; however, since the majority of children with developmental disorders appear intellectually normal and the number of such children is not negligible (which I will discuss later), the establishment of a new educational framework called 'special needs education' has become an urgent issue (Figure 3).
What is a developmental disorder?
What exactly is a developmental disorder? Children with a developmental disorder are often identified as showing 'unusual' behavior among other children at kindergarten, the daycare center, or elementary school. Then, what is unusual behavior? Figures 4, 5, and 6 summarize the unusual behavior patterns of children. Although these children have no intellectual disability, they share similar behavior patterns such as the difficulty of participating in group activities, listening to the teacher's instructions, and controlling their emotions. They may also find it difficult to understand others' feelings or social rules and contexts.
Figure 4: Children under caution
A child in need of special attention:- has difficulty listening to the teacher's instructions
- has difficulty playing within a group of children
- has difficulty participating in group activities
- often behaves impulsively
- has difficulty maintaining daily habits and practices
- has difficulty following social rules
- has difficulty understanding and expressing social communication cues
Figure 5: Unusual behavior of young children
In a group, the child ...- is restless and fidgety
- often causes trouble with friends
- often loses things
- tends to break off from a group
- often has difficulty playing with other children
- cries easily
- often has difficulty following the flow of a conversation
- often exhibits social awkwardness and clumsiness
- does not like to play with neighborhood children
- is a picky eater
- avoids interaction with other adults except parents
- has rapid mood swings
- often be thought to be selfish
- often has difficulty keeping a daily rhythm
- likes to repeat the same thing over and over again
- often has poor manners
(by clinical psychotherapist Masako Okada)
Figure 6: Unusual behavior of children in group
Problems:- Has difficulty following the teacher's instructions
- Has difficulty sitting still
- Talks excessively
- Often fights with other children
- Cries easily and makes excessive noise
- Has difficulty concentrating and paying attention
- Is passive and inattentive
- Often shows immature behavior for a child of his/her age
- Has difficulty in making and sustaining friendships, although he/she can get along with the teacher
(by clinical psychotherapist Masako Okada)
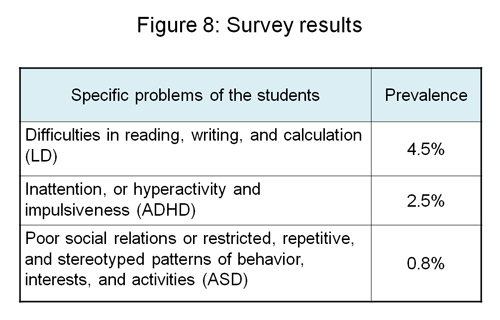
It should be noted that the unusual behavior of children is not always due to a developmental disorder, yet for some children, this is the cause of their behavior. This fact is also supported by the survey conducted by the Ministry of Education, Culture, Sports, Science and Technology (MEXT) in 2003 (Figures 7 and 8). The survey revealed that a significant percentage of children (6.3%) in normal classes would be diagnosed with a developmental disorder. The percentage of children with intellectual or physical disabilities is said to be approximately 2%; therefore, the number of children who require special needs education is several times higher than those eligible for the conventional special education services.
Figure 7: Survey on developmental disorders in Japan
This survey was conducted by the Ministry of Education, Culture, Sports, Science and Technology in 2002- Subject: 41,579 children in 370 public elementary and junior-high schools
- Evaluation criteria for teachers: Criteria for ADHD, LD and autism
- Data-collection rate: 98.6%
Attention deficit hyperactivity disorder (ADHD)
The highest percentage of attention deficit hyperactivity disorder (ADHD) is found among children with developmental disorders. In the survey, the MEXT estimates that the number of children with ADHD accounts for 2.5% of the total number of children; however, the rate is relatively higher in many other countries. For example, according to a survey conducted in the USA, 8% of children in the country have been diagnosed with ADHD, a much higher rate than that in Japan. It is more common in boys than girls, one of the typical characteristics of developmental disorders, with a male-to-female ratio of 4-5 to 1. ADHD diagnosis is based on the number of symptoms under the criteria defined in the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, fourth edition). If a child shows several symptoms that exceed a certain level (e.g., six or more symptoms), and if the child has difficulty with activities at school and home due to such symptoms, then the child is diagnosed with ADHD. These symptoms include the following: often fidgets with hands or feet or squirms in while sitting; often leaves his or her seat in classroom or in other situations in which remaining seated is expected; often blurts out answers before questions have been completed; often loses things necessary for tasks or activities; is often forgetful in daily activities; often has difficulty awaiting turn; and often has difficulty organizing tasks and activities.
Since children with such symptoms can easily become the subject of scolding, bullying or teasing and tend to have feelings of low self-esteem, they are at high risk of developing a secondary disability such as depression and conduct disorders. Or they may suffer from comorbid disorders such as learning disabilities in reading, writing and mastering calculations, or a pervasive developmental disorder (see the next chapter), which are also quite common in ADHD children.
There are several behavioral treatments proven to be effective for ADHD; for example, changing the classroom environment to promote better concentration, avoiding scolding and giving positive praise when they act appropriately. In addition, medication with methylphenidate or atomoxetine has been proven to be effective and popular for the treatment of ADHD symptoms.
High-functioning autism, Asperger's syndrome, and learning disabilities
High-functioning autism (HFA) and Asperger's syndrome (AS) are classified in the category of pervasive developmental disorders, one within the range of the developmental disorders. Unlike ADHD, the diagnostic characteristic of HFA and AS is significant difficulty in developing interpersonal relationships, since people with HFA or AS are developmentally delayed in interpreting others' moods and feelings from their facial expressions and verbal cues. They may have a speech delay, and take what people say very literally and have problems understanding more complicated implications such as irony and sarcasm. Therefore, they find it difficult to make and keep friends and tend to have poor peer relationships. They are also painfully sensitive to certain sounds and situations that may cause nervousness or panic attacks. At the same time, people with HFA or AS show a strong interest in a particular topic, such as timetables and calendars, even memorize entire passages from a favorite picture book. When talking with others, they just talk about things that interest them, without knowing what others might be interested in. These symptoms make it very hard for them to make friends.
A learning disability is one of the developmental disorders where children have no intellectual disability but a significant delay in literacy performance, such as reading, writing and comprehending the contextual meaning of text. Children with a learning disability are often identified after they start elementary school; but at the beginning, their poor performance in class is often misinterpreted as laziness.
Common symptoms of developmental disorders and neuroscience
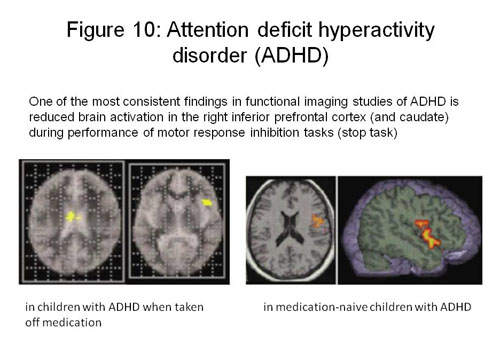
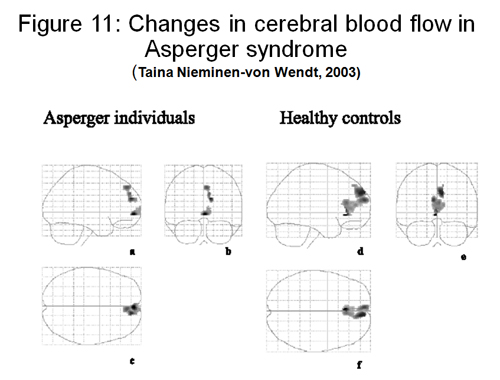
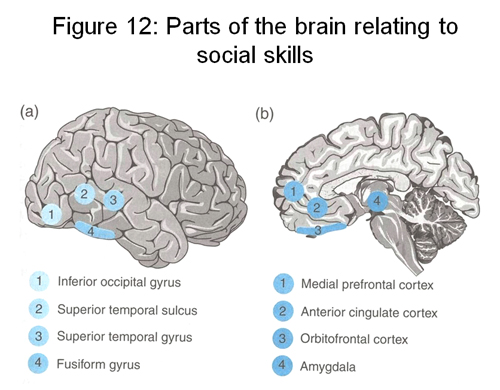
Figure 9 summarizes the common symptoms of developmental disorders. All of them are not caused by poor parenting or the child's attitudes, but due to an innate malfunction of certain parts of the brain, or more medically speaking, insufficient activation in the brain that causes the impaired brain function. Figures 10, 11, 12 and 13 show images of deterioration in brain function produced by the functional brain imaging technique. A decreased level of activity can be seen in the frontal lobes and caudate nucleus in ADHD, and in the frontal and temporal lobes in HFA and AS (the temporal lobes are involved in the primary organization of sensory input such as reading facial expressions, whereas the frontal lobes play an important part in understanding and appreciating the feelings of others). In the case of people with a learning disability, reduced activity is observed within the brain's neural network which affects the ability to understand written words.
Figure 9: Common symptoms of developmental disorders
Developmental disorders are...- inborn disorders
- genetically transferred and passed on by heredity in some cases
- not associated with intellectual disabilities
- more common in boys than girls
- often identified when the child participates in group activities at school/kindergarten
- often associated with comorbid/secondary disorders
- have a high prevalence rate (up to 10%)
- result from abnormal activities in the brain that can be detected by a functional brain imaging test
Measures taken by school and kindergarten to help children with developmental disorders
Developmental disorders are not rare: children with developmental disorders account for 6.3% of the total population of children. It has become more widely recognized by the general public that teaching and taking care of children who display symptoms of developmental disorders should not be left to a limited number of staff members at school and kindergarten; rather, it is preferable that every teacher learn about and understand developmental disorders and their basic treatments. Figures 14, 15, 16 and 17 show conceptual diagrams of special needs education in Japan.
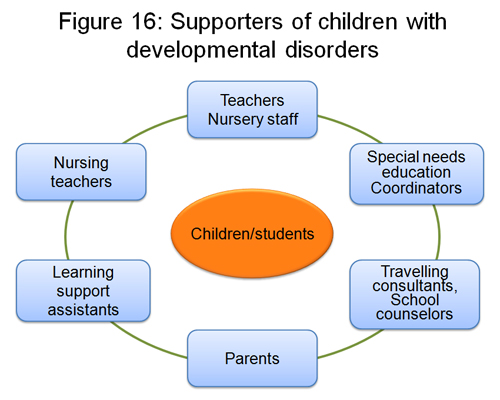
The Japanese law requires every school to establish an internal committee and coordinators for special needs education. It is essential that not only school members but also specialists for child development, psychology, medical science and welfare collaborate as a team to support children with developmental disorders.











