

I. Alcohol metabolism in a mother's body and her fetus
Alcohol consumption in any amount by pregnant women cannot be considered safe for the fetus. Although a causal linkage between the quantity and duration of alcohol consumption, phase of pregnancy, and fetotoxic effect has not yet been established, there is no room for doubt that the concept of low risk and responsible drinking does not apply to pregnant women. The fetus is safest when the mother abstains from drink. However, it is estimated that more than 10 percent of women choose to continue drinking during pregnancy.
When alcohol is consumed, it is absorbed into the bloodstream through the digestive tract, and acetaldehyde is formed mainly by the oxidation of alcohol dehydrogenase (ADH) in the liver. Then acetaldehyde dehydrogenase (ALDH) converts this acetaldehyde to acetic acid. Acetic acid undergoes several and complex routes, and is finally broken down into H2O and CO2 which are discharged to the outside of the body.
The alcohol metabolism of a pregnant woman is much depressed compared with that of a non-pregnant woman, as estrogens largely inhibit the activity of ADH and ALDH, especially estradiol, one of three principle forms of estrogens, which has the strongest effect. Moreover, the total amount of estrogens in the serum of a pregnant woman in the early stages of pregnancy will increase by 10 - 100 times compared to that of a non-pregnant woman, and in mid to late pregnancy, increase by 100 - 1000 times. This affects the alcohol metabolism of a pregnant woman, and each of the three main estrogens exhibit relatively more volatility.
In terms of the alcohol metabolism in the body, there is no feedback mechanism and the metabolic rate is stable, 7g per hour. Generally, each of one medium size of bottle of beer (500ml), one goh of Japanese sake (180ml), two glasses of wine (240ml), two fifth goh of shochu (distilled spirit, 70ml), or one double whisky or brandy (60ml) contains 20g of alcohol. Therefore, the time required for the completion of alcohol metabolism when several kinds of alcohol are consumed can be estimated by dividing the total amount of alcohol consumption (g) by 7g. For a pregnant woman, this estimated time should be multiplied by 1.5. For example, when a person drinks one medium bottle of beer and two goh of Japanese sake, total amount of alcohol consumed will be 20g + (two goh × 20g) = 60g. Thus the required time for alcohol metabolism for this person will be 60g / 7g = 8.6 hours, and in case of pregnant woman, 8.6 × 1.5 = 13 hours.
A pregnant woman is physiologically in a state of dynamic equilibrium along with the development of fetus, therefore, her condition places her at a disadvantage for the efficient metabolism of alcohol. ADH can be found in a fetal liver from the middle of the third month of pregnancy, and its activity will slightly linear increase; nonetheless, a fetus has almost no capacity to break down alcohol. In addition, a low molecular weight alcohol passes swiftly through the placenta and harms a developing fetus. Fifty percent of the alcohol crossing the placenta enters the bloodstream of the fetus, and the remaining 50% enters the circulatory system via the fetal liver. While alcohol remains in the bloodstream, the fetus, so to speak, continues being forced to consume alcohol by the mother.
Forty percent of pregnant women addicted to alcohol give birth to a baby with Fetal Alcohol Syndrome (FAS). In Japan, Dr. Takashima and others presented the first case in 1978. Both FAS as well as FAE (Fetal Alcohol Effects, incomplete features of FAS) are considered to be caused mainly by the direct action of alcohol (ethanol). There are also cases of suspected FAS (potential group) without any apparent symptoms. Three main diagnostic terms are used to describe babies associated with FAS caused by prenatal exposure to alcohol: facial abnormalities, dysfunction of the central nervous system, and retardation of growth.
Dr. Rosett standardized the diagnostic criteria(1) for FAS as shown below;
- Prenatal and/or postnatal growth deficiency, if any one or more of weight, length, or head circumference are below the 10th percentile.
- Central nervous system (CNS) disorders, including at least one of the following: neurological abnormality, developmental delay, and intellectual impairment.
- A distinctive pattern of facial anomalies, including at least any two of microcephalia; microphthalmia and /or short palpebral fissures (eye slits); an indistinct philtrum; a thin upper lip; and an elongated, flattened midface (the zone between the nose and the mouth).
If symptoms are found in all of 1, 2, 3 categories above, the baby is suspected to have FAS, and if symptoms are found in any of 1, 2, 3 categories, then suspected to have FAE. Meanwhile, Dr. Streissguth (2000) proposed the concept of Fetal Alcohol Spectrum Disorder (FASD), a continuum of permanent birth defects caused by maternal consumption of alcohol during pregnancy.
In Japan, the estimated rate of FAS at birth was 1 per 1,000 births 30 years ago, and the current rate must be lower than 10% of that. However, this rate may vary considerably depending on the living standard of local communities.
A fetus by the 8th week of pregnancy is still called an embryo. This embryonic period is the critical time when the fetal organs are most susceptible to the development of major abnormalities caused by the fetotoxic effect of alcohol. Susceptibility to alcohol regarding whole organs or a part shows individual variability. Thalidomide, a notorious sleep-inducing drug, causes birth defects if a pregnant woman takes the drug at a certain stage of the embryonic period (34th - 50th day after the first day of the last menstrual period). In contrast, alcohol exposure can cause damage to fetus at all stages of in utero development. The effects of fetal toxicity on development of the fetal organs occur mainly at the early stage of pregnancy including the embryonic period, and on the entire growth of the fetus at the period of mid to late pregnancy. Thus, it can be said that FAS (FAE) is embryopathy and at the same time, fetopathy. FAS is not an accidental disease; this is just the tip of the iceberg, below the surface there are enormous hidden problems.
More specifically, the embryo or fetus in a pregnant woman who continues drinking will sustain fatal damage and miscarry as a process of natural selection. However, if this damage is limited and not fatal to the embryo or fetus, it will remain in the womb due to the anti-miscarriage effect of alcohol and continue to develop. Nevertheless, the development of the entire fetus will be inhibited if the mother continues drinking. As a result, some babies are born with clinically evident congenital abnormalities (FAS) and some with several suspected abnormalities but no apparent symptoms.
III. Prenatal treatment
In the light of recent advances in testing techniques and instrumentation such as an ultrasonotomography, it seems that prenatal treatment(2) has some potential for a fetus exposed to alcohol, but is still unrealizable today. For a baby born with a congenital anomaly, this means receiving appropriate child-care. A Fetal Alcohol Syndrome Screening test (FAST)(3) (Table 1) can be used for embryo screening. However, this test should be practiced to help determine risk for abnormalities of a fetus or newborn baby, but never in order to recommend an induced abortion. It is useful to refer to FAST to prepare the specific instruments for parturition in advance, because a pregnant woman who drinks alcohol quite often needs an obstetric operation during the intrapartum period.(4) FAST data can be applied as reference after childbirth as well. There is also the problem drinking screening chart for pregnant women as shown below(5) (Figure 1), a combination of the FAST method and the Kurihama Alcoholism Screening Test (KAST)(6) (Table 2) to be used at the time of pregnancy or labor.
While the problem drinking screening chart for pregnant women(5) will identify the alcoholic pregnant woman, the DSM-IV, an alcohol dependence diagnosis, defines alcohol abuse as follows (quote Higuchi's chart(7) in part).
Alcohol use with clinically significant impairment is indicated by at least three of the following seven items within any one-year period: 1. tolerance; 2. withdrawal; 3. loss of the ability to have control over drinking; 4. unsuccessful attempts or desire to reduce or control drinking; 5. great deal of time spent drinking or recovering from drinking; 6. decrease in social, occupational, or recreational activities that are not centered on drinking; 7. resistance to negative reinforcement.
The typical process of becoming an alcoholic is considered as follows: first-time drinking --> occasional drinking --> habitual drinking --> wider repertoire of drinks (succumb to any kind of alcohol) --> search for alcohol (find out and drink even hidden alcohol) --> become a strong drinker --> repeat withdrawals --> drink alcohol to avoid withdrawals --> intense desire to drink --> abnormal drinking (continuous drinking).
<Figure 1>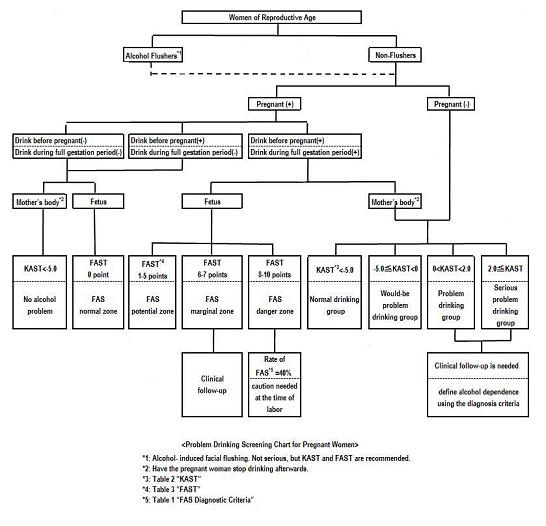
Enlarge
<Table 1>
<Table 2>
References
| 1) | Rosett, H.L.(1980): A clinical perspective of the fetal alcohol syndrome. Alcoholism., 4: 119 |
| 2) | Yoichi Niimi (1990): Prenatal treatment for fetal alcohol syndrome - Present condition of approach to prenatal treatment, Research on medical care for alcoholic, 7:45 |
| 3) | Yoichi Niimi, Taro Matsumura, et al. (1989): FAS screening test for fetus and new-born baby (FAST) by diagnostic process with an interview with the patient, Research on medical care for alcoholic, 6:207 |
| 4) | Yoichi Niimi (1975): Statistical considerations in women with alcohol preference in child birth, Obstetrics and gynecology, 42:9 |
| 5) | Yoichi Niimi (1994): Pregnant women and drinking alcohol, Gynecology medical treatment, 68:773 |
| 6) | Saito, S., Ikegami, N. (1978): KAST (Kurihama Alcoholism Screening Test) and its applications, Japan J. Stud. Alcohol., 13:229 |
| 7) | Susumu Higuchi (2003): An introduction to alcohol addiction, Separate volume, Psychiatric syndrome III, Nippon Rinsho, 405 |











